- Functional Unit is the Hepatic Lobule (-->Ascinis --> portal triad)
- 50-100 K present in normal liver
- Primary blood supply is the Hepatic Artery (30%) and Portal Vein (70%) representing 30% of cardiac output
- As the blood supply is from the gut, it contains large numbers of colonic bacilli
- primary physiologic function
- bacterial cleansing (99% of the load) is cleansed by the macrophages (Kupffer's Cells) lining the hepatic sinuses
- endothelial cells also line the hepatic sinuses. They are permeable to large plasma proteins allowing to move freely into the extravascular spaces of the liver.
- phagocytize bacteria
- cell ghosts
Responsible for:
- processing antigens
- release of some proteins, cytokines and mediators
- removes bacteria, endotoxins, cellular debris, viruses, proteins, and other cellular garbage from portal circulation
- inflammatory mediators
- shit that comes from the gut (mesenteric and splenic veins)
- pulls out nutrients and proteins that we eat

Stellate cell = Ito cell (become fibrotic in inflammatory process; proliferate, fill up Space of Dise; lumen of vessel shrinks and encapsulate vasculature. Normal pressure of portal vein is 7-10 mmHg [low pressure high flow system - similar to lungs])

- Glucose absorbed postprandial (after meals)
- Stored as glycogen
- Sites of glycogen storage: muscle & liver
- When storage is maximized, excess glucose is converted to fat (adipose)
- Insulin enhances glycogen manufacture by the liver as does: glucocorticoids, thyroid hormone, epinephrine
- Epinephrine encourages glycogenolysis
- The liberation of liver glycogen for energy source (Glucagon as well)
- Glycogen storage is approximately 70gm (max)
- Daily requirements are twice that
- Glycogen stores are depleted after 24 hours of fasting
- start using ketones from fat
- Gluconeogenesis helps maintain normal BG levels (neo source; from a non carbohydrate source, usually lactate but also protein and fat)
- excess CHO are converted to fat when storage is maximized
- fatty acids can then be used immediately for fuel or stored in tissue (3x as many calories from fat than from CHO)
- RBCs and renal medulla are unique in that they can utilized only glucose as energy source
- neurons in CNS utilized only glucose under normal conditions
- in starvation states neurons can switch their metabolic machinery to break down ketone bodies, the result of anaerobic metabolism
- Acetoacetate is the favorite ketone of the liver
- converted to Acetyl-CoA for energy and to act as a substrate for building cellular membranes and organelles
- Deamination of amino acids (taking apart amino acids)
- Converts AA to ketoacids producing an ammonia byproduct
- Formation of urea from toxic and ammonia: produced here and in gut by enteric flora
- Formation of plasma proteins:
- Quantitative priorities (need volumes of them):
- Albumin (& gamma globulins)
- alpha-1 antitrypsin
- other protease-elastases
- Qualitative priorities:
- coagulation factors
- All factors but F 8 and von Willebrand Factor produced by the liver
- tissue factor (F3) synthesized by endothelial tissue (= platelet tissue factor)
- The first sign of reduced hepatic synthesis: PT - prothrombin time increases
- albumin level decreasing is NOT an early sign bc 1/2 life is 14-20 days
- hypoalbuminemia is a chronic sign
- Inducible --> can make those things work harder (ETOH)
- "enzyme induced"
- "circulation time"
- oxidation/reduction reactions
- Identify the patient that may require more drug/less drug? enzyme induced
- Identifying agent that inhibits 450 oxidase
- identify a breakfast drink that does the same - grapefruit juice, watercress
- What does the high hepatic extraction rate of morphine, lidocaine, and trandate mean to you?
- high extraction rate: significantly drops the dose (we need to give more drugs)
- Don't necessarily follow phase 1 reactions
- become more polarized
- fentanyl - fat - lipid soluble; liver conjugates it to a water soluble product
- generally involve conjugation with:
- glucuronide - primary conjugator
- sulfate
- glycine
Volatile agents will decrease blood flow
Halothane by up to 25%, and abolishes the vasoconstrictive response to increase CO2
Hepatic artery has capacity to vasoconstrict and vasodilate; portal vein cannot
- bile production
- insulin clearance
- lactate conversion to glucose (gluconeogenesis)
- also from Alanine and Glycerol
- drug metabolism and transformation
- degradation of insulin
- hormone metabolism
- Thyroxin (liver) --> trithyroiodine, more active form
- men develop feminine characteristics in hepatic disease
- ADH, thyroid, glucagon, aldosterone, cortisol & estrogen
- Vitamin storage in hepatocytes (A, B12, E & D)
- Transferrin and heptoglobin synthesis effects Fe metabolism
- Ceruloplasmin necessary for copper metabolism (Wilson's disease - 10% of hepatic transplants - women; neuropsych issues; copper accumulates in basal ganglia; copper in eyes - kaiser flasher ring)
- A, D, E, K - fat soluble vitamins - a duck eats kake
- blood supply to liver: hepatic artery and portal vein --> hepatic sinusoidal channels, serving as capillaries
- endothelial cells and Kupffer's cells line the sinusoids
- bile canaliculi, between the hepatocytes, empty into terminal bile ducts
- Hepatocytes surround the central veins, empty to hepatic veins, emptying into inferior Vena Cava
- extensive arcade of lymph channels are present within the layer of cells
- Primary secretion of liver
- 1 L/day produced by hepatocytes
- contains phospholipids, cholesterold, conjugated bilirubin: end product of Hgb breakdown
- stored & concentrated in gall bladder (5-12x), released under influence to CCK into duodenum via Sphincter of Oddi
- Aids in absorption of fat and fat soluble vitamins (ADEK)
- metabolic end products of drug metabolism removed via bile
- liver disease results in delayed bile production and/or flow
- resulting in steatorrhea (fatty stool)
- Vitamine K deficiency
- delayed removal of active drug metabolites
- All factors produced by liver except F8 and vWF produced by endothelial cells
- 50% liver function necessary for normal clotting factor production
- impaired bile production results in decreased bile production impairing production of Vitamin K dependent clotting factors (2, 7, 9, 10)
- Only need to replace FFP up to 50% (not 100%)
- Intrahepatic obstruction to blood flow results in portal HTN
- congestive splenomegaly
- sequestration thrombocytopenia (spleen captures platelets)
- inducing coagulopathy
- Due to:
- impaired coagulation factors
- diminution of circulating functioning platelets (left over plts don't work well)
- Parenteral (injected) Vitamin K --> IM
- significant disease may require administration of FFP and platelets
- subarachnoid and epidural are not done in presence of frank coagulopahty-->subarachnoid hematoma
- instrumentation of nasopharynx (NGT) or any invasive procedure must be approached cautiously in presence of clotting derangement (esophageal varices) - Afrin/oxymethazole
- all proteins except some immunoglobulin's produced in liver
- low protein level
- low plasma oncotic pressure
- decreased drug binding in highly protein bound drugs (barbiturates, versed)
- may result in exaggerated effect of these drugs
- plasma oncotic pressures shifts results in large volume of distribution of drug
- increased VD may result in need for increased dosing of NDMR (higher initial dose and lower redose)
- VD curve is skewed
- Rx ends up in ascites
- produced by liver
- may be dificient in disease states
- cholinesterase deficiency prolongs: Succs, Mivacurium
- Also may enhance the potential toxity of Ester LA: tetracaine, procaine, chloroprocaine and cocaine
- metabolized by PC
Phase 1 Reactions: oxidation/reduction reactions, deamination, methylation, hydrolysis
Phase 2 Reactions: conjugation with glycine, sulfates, glucuronide, then ready for elimination in bile or urine
- overproduction of CYP450 system results in increased hepatic enzymes
- Causes:
- ETOH
- Benzodiazapines
- Ketamine
- Barbiturates
- Result: increased requirement for sedatives, opioids, neuromuscular blockers
- decreases the activity of these enzymes, increasing the effect of some anesthetic agents, potentially prolonging wake up
- same thing with grapefruit juice
HEPATIC DISEASES:
Caused by an interruption of biliary release
Most common causes:
- gallstones obstructing the common bile duct
- pancreatic CA
- parasites (liver flukes) can set up housekeeping in the common duct causing obstruction
- biliary atresia (blind pouch) - no outlet for gallbladder
- ductal or ampullary carcinoma
- pancreatitis - gall stones (cholesterol stones) block pancreatic duct - autodigestion
- pancreatic pseudocyst (not a complete wall) not a carcinoma - can rupture and aspirate pancreatic bolus of digestive enzymes --> RSI
*narcotic can cause sphinter of Oddi spasm - but not a big deal; glucagon
HEPATITIS
- Short incubation: 15-45 days
- Acute onset
- highly contagious carried by hands, feces of infected carriers, or contaminated shell fish
- may be transmitted by IV drug users and sexual contact
- virus is shed in stool for up to 3 weeks before the onset of jaundice
- immune globulin and Hep A vaccine provide immunity
- does NOT lead to chronic liver disease
- Long incubation: 45-160 days
- subtle onset
- often very sick
- chronicity - children 80%, Adults 5%
- transmission via infected blood products, bodily fluids or sexual contact with asymptomatic carrier
- large population has serum antibodies conferring immunity to Hepatitis B
- up to 30% may be asymptomatic infectious carrier as B surface antigen persists in the patients blood (HBs Ag)
- post-exposure prophylaxis with hyperimmune globulin injection is effective for HBV but not HCV
- infectivity correlates with the amount of viral RNA in patient's blood
- infection confers immunity to further HBV infections
- Incubation: 30-70 days
- transmitted via parenteral routes, blood products, occupational exposure and IV drug use
- may be transmitted by razors and toothbrushes
- most common blood born infection in US
- blood is screened for HCV and transmission rates are low
- perinatal infection mom to fetus rates are also low
- depends on the viral load
- Formerly known as Non A Non B
- 1% become asymptomatic infectious carriers
- predominant liver disease in USA
- HCV progression to end stage liver disease is slow - cirrhosis in 20 yrs --> cancer
- HCV is the leading indication for hepatic transplant (OLT)
- HCV cirrhosis also responsible for large numbers of hepatocellular cancers (hepatoma)
- HDV occurs only in patients with coexisting Hepatitis B and worsens the symptoms
- you are protected from HDV if you have immunity to HBV
- Enteric Non A-Non B
- transmitted via oral fecal route
- not found in USA
- Gradual or sudden
- dark urine, fatigue, anorexia, nausea, fever, headache, abdominal discomfort
- pruritis
- jaundice (but could be getting better) --> icteric; scleral icteris in dark-skin ppl
- acholic or clay colored stools
- Symptomatic and supportive care
- HCV interferon with ribaviron administered
- may rarely develop encephalopathy and coagulopathy necessitating hepatic transplant
- administer gamma globulin and give vaccine within 24 hours of exposure (with Hep A or B)
- for Hep C there is nothing you can do that will statistically change outcomes; routinely given ribaviron
- CMV: cytomegalovirus; Epstein-Barr Virus (mononucleosis - kissing disease)
- Herpes Simplex - Coxsackievirus
- VAAs - any drug that decreases hepatic blood flow - Halothane....Sevo is the safest
- drug induced hepatitis indigtinguishable from acute viral hepatitis
- N/V - 2 weeks
- Jaundice if it occurs when viral titers peak - last up to 12 weeks
- return of serum transaminase to normal levels - possibly 4 months to return to normal
LABORATORY ANALYSIS OF LIVER FUNCTION
In its original form, bilirubin is fat soluble
Glucuronyl transferase modifies bilirubin as it arrives at the liver and converts it to a water solube compound
This process is called bilirubin conjugation as bilirubin is attached to a water molecule
Green substance in bilirubin --> biliverdin
Bilirubin is yellow
- conjugated bilirubin is then excreted into the bile and is released into the gut
- impairment of any of these steps results in distribution of bilirubin, unconjugated, conjugated or both throughout the body
- unconjugated bilirubin (fat soluble) accumulates in fatty tissues, most notably in the skin
- the presence of this yellow pigment produces jaundice
- increased RBC breakdown - prehepatic
- failure of hepatocyte conjugation - hepatic
- failure of hepatocyte excretion of conjugated bilirubin into the bile canaliculi - hepatic
- extrahepatic obstruction (gallstones) - post hepatic
Marked elevation may signal:
- prehepatic --> hemolytic process
- hepatic --> failure of conjugation (parenchymal disease) unique to organ; excretion into canniliculi is blocked - goes to spaces of dise and lymph channels --> high conjugated bilirubin, acholic stools
- post hepatic obstruction --> extrahepatic obstruction
- *ALT more specific indicator of liver damage compared to AST
- Always Liver Toxic (ALT)
- Normal range: 10-55 u/L
- Circulating T1/2 about 24 hours
- Nonspecific indicator of tissue damage
- also found in brain, pancrease, and heart
- Alternate source toxin - From somewhere else that has inflammation
- Normal range: 10-40 u/L
- Circulating T1/2 about 24 hours
- AST/ALT > 2 suggests alcoholic liver disease or cirrhosis of any cause
- May be elevated in many types of liver disease, extra or intrahepatic cholestasis or liver tumor - released from ductal cells in inflammation
- found in disease involving bone growth and Paget's disease and intestinal tumors
- found in normal states involving growth: children and teens experiencing rapid growth; prenancy
- Normal: 45-115 u/L
- Circulating T 1/2 is 7 days
- AP = Also Paget's disease
- Normal range: 0-30 u/L
- stimulated by many of the intrahepatic factors that stimulate alkaline phosphatase
- used as a marker for alcoholic liver disease GGTP/AP > 2.5 suggest alcoholic liver disease
- also found in kidney, spleen, pancreas, heart
- Get Granny the Pabst (Blue Ribbon)
Allows separation of hepatobiliary isoenzymes from other isoenzymes (5NT and LAP found elevated in third trimester)
- Normal values: 11-12.5 seconds
- INR: 0.9 to 1.2
- PT is the first marker in acute liver disease to decline
- prolongation represents a decreased synthetic capacity of the liver
- PT factors: 1, 2, 5, 7, 10
- If PT is unresponsive to vitamin K, liver failure exists
- extra hepatic prolongation may occur in Vit K deficiencies
- Causes: malabsorption, malnutrition, long term antibiotics
- Normal values: 3.5-5 g/dL
- low albumin levels represent the livers' decreased ability to synthesize albumin as seen in chronic liver failure
- extra hepatic influences of hypoalbuminemia: malnutrition malignancy, infection, nephritic syndrome (protein and RBC loss)
- albumin produced by the liver - easily measured and is main constituent of total protein
- the remaining fraction is called globulin (including the immunoglobulin)
- albumin levels are decreased in chronic liver disease, such as cirrhosis
- also decreased in nephritic and nephrotic syndrome where it is lost through urine
- poor nutrition and protein catabolism may also lead to hypoalbuminemia
- T1/2 is approx 20 days
- Elevation reflects a disruption of hepatic urea synthesis
- Normal: 82-110 mg/dL or 47-65 mmol/L
- reflective of severe hepatocellular damage
- ammonia levels do not correlate well with level of cellular destruction
CIRRHOSIS
The end result of a variety of progressive liver disease
Commonly: - ETOH
- HBV
- HCV
- alcoholic cirrhosis (Laennec's cirrhosis)
- scarring and fibrosis disrupts the liver architecture
- unequivocal diagnosis: liver biopsy
- Guidelines: INR < 1.5, Platelets > 50,000
- splenomegaly
- ascites
- irregular enlarged liver an early sign
- small hard liver a late sign d/t contracted fibrotic organ
- spider nevi
- gynecomastia
- testicular atrophy
- portal HTN
- ascites & splenomegaly are characteristics of cirrhosis but not diagnostic
- Halothane: trifluroacetyl metabolites - autoimmune
- Sevo does NOT generate trifluroacetyl metabolites
- Halothane significantly decreases blood flow to liver
- causes profound hepatocellular necrosis
- glutathione stores are exhausted
- **toxic metabolite is unable to be conjugated for excretion
- treatment: supportive
- Administer N-acetylcysteine (Mucomyst) via NGT - precursor to glutathione
- phase 1 metabolism - 20% of end product is toxic
- results not from Acetaminophen directly
- actually from its Phase I metabolite: N-acetyle-P-benzoquinoloneimine (NAPQI) also known as "Toxic Metabolite"
- Moving to phase II - glutathione stores are rapidly depleted
- direct hepatocellular damage occurs and irreversible liver damage results
- ETOH, ASA, tylenol, Shrooms
- Idiosyncratic: Halothane, Phenytoin, Indomethacin, Sulfonamides
- Primary cholestatic: chlorpromazine, oral contraceptive, anabolic steroids, e-mycin and methimazole

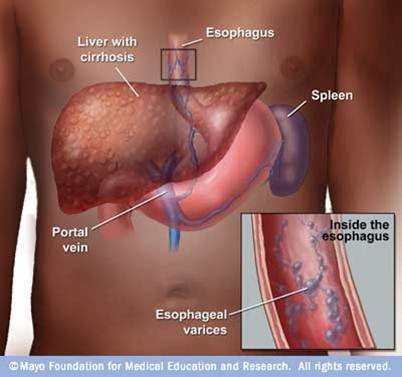
BLOOD FLOW IN PORTAL HYPERTENSION
TYPES OF CIRRHOSIS:
Primary Biliary Cirrhosis: autoimmune; occurs in women 30-50 y/o
Hemochromatosis: a disease of iron (Fe) deposition; DM and cardiomyopathic problems; die of CA
Wilson's Disease: hepatolenticular degeneration; neuro and hepatic dysfunction d/t copper metabolism error; copper desposited into basal ganglia --> mood swings and depression (10% of liver transplants); Kayser Fleischer ring (copper) around pts eyes
Non-Alcoholic Steatohepatitis: may occur with obesity, hyperlipidemia and diabetes mellitus; Fatty accumulation occurs in liver. Steato = fat
COMPLICATIONS OF CIRRHOSIS
- Portal HTN
- Gastroesophageal Varices: submucosal veins dilate d/t high pressure portal blood flow to low pressure azygoes and hemizygous thoracic veins
- Bleeding may be significant
- Diagnosis: EGD, may band - not usually intubated unless ascites is significant or actively bleeding
- Hemorrhoids also d/t shunting of hyperdynamic blood flow to low pressure areas; not a life threatening issue, but unpleasant for patient (and clinician)
- Hepatorenal syndrome: usually fatal d/t decreased blood flow and markedly reduced GFR
- malnutrition
- arterial hypoxemia
- d/t ammonia accumulation
- presence of ascites inhibiting diaphragmatic excursion
- hyperdynamic shunting
- hypoglycemia d/t inefficient glycogen stores
- formation of gallstones (cholelithiasis) - obstruct pancreas --> pancreatitis
- bleeding from duodenal ulcers
- hepatic encephalopathy (ammonia levels)
- asterixis --> liver flap/twitching
- not able to metabolize insulin
- Dupuytren's contractures
- impaired estrogen metabolism
- Postpone surgery until lab values return to normal
- periop morbidity increases 12% and mortality increase 10% (with laparotomy) during acute viral hepatitis episodes
- Postop, hepatitis patients are at risk for:
- fulminant hepatic failure
- encephalopathy
- coagulopathy
- hepatic renal syndrome
- Objective: decrease the periop mortality and morbidity associated with liver dysfunction
- identify cardio respiratory dysfunction
- alcoholic cardiomyopathy
- coagulopathy
- renal function
- assess IV volume
- lab analysis
- nutrition issues
- PT is best indicator of hepatic synthetic function
- if PT prolonged > 3 sec or INR > 1.5 following vit K admin, severe hepatic dysfunction is present
- vit K usually beneficial in the presence of obstructive biliary disease (post hepatic) as opposed to parenchymal disease (hepatic)
- bile salts are needed to facilitate absorption of vit K in gut
- may need FFR/ platelets
- evaluate blood glucose levels: generally labile
- other comorbidities
- Perform serum ETOH level if you suspect ETOH consumption
- alcohol withdrawal presents mortalities as high as 50%; only true emergencies should be considered
- alcoholic patients present cross tolerance to anesthetic agents
- requires close CV monitoring d/t cardiac depressant effects of ETOH and anesthetic agents
- alcoholic cardiomyopathy may be present
- VAAs, d/t their decreased metabolic profile, are preferred over IV agents
- isoflurane has lowest effect on renal blood flow and hepatic blood flow; agent of choice
- IV induction doses are ok as their action is terminated by redistribution not metabolism
- Be aware of prolonged duration of action with repeated doses
- avoid hypotension, SANS stim & high peak airway pressures in order to maintain steady-state hepatic blood flow
- regional anesthesia may be employed in the absence of coagulopathy if arterial hypotension is avoided
- Hepatic blood flow already decreased in this patient
- d/t increased resistence to blood flow via portal vein
- anesthetic induced depression of cardiac output or hypotension may jeopardize hepatic blood flow
- be prepared for possible impaired response to catecholamines in presence of acute surgical blood loss
- low protein levels promotes an increase in the pharmacological active fractions of injected drugs
- more drug available to receptor sites
- severely jaundiced patients are more likely to develop sepsis and renal failure postop
- Serum bilirubin > 8 mg/dl
- Rx: diuresis with mannitol and antibiotic therapy
- hepatic artery becomes more important now as this vessel can dilate in response to decreases in portal blood flow
- hepatocyte oxygenation is maintained with Iso, Sevo, and Des, but NOT halothane
- limit dose but give what is needed
- supplement with N2O and IV agents as appropriate
- maintain BP; hypotension correlates with incr mortality
- cumulative drug effect may be enhanced d/t decreased hepatic metabolism
- Vec not a clearance problem until dose exceeds 0.1 mg/kg
- Miva, Atra, and cisatra are good choices (non-organ dependent elimination)
- stress induced SANS stim decreases hepatocyte O2
- Monitor ABG: portosystemic and intrapulmonary shunts dilate in response to anesthetic agents = hypoxemia
- CVP and PAC may be necessary to eval volume status
- monitor blood glucose
- admin glucose containing infusions as necessary
- glucose containing solutions are hepatocyte sparing
- when giving blood products:
- give slowly
- citrate is not cleared by liver and may precipitate hypocalcemia and hypotension
- maintain UOP to help reduce the incidence of postop renal failure; give mannitol to establish diuresis & free radical scavenger
- avoid unnecessary esophageal instrumentation: temp probe, stethoscope, OGT
- avoid nasal instrumentation
- preop discussion should include:
- large bore IV access
- invasive monitoring
- blood and blood products
- portocaval shunt procedures usually require full invasive lines (aline, CVP, PAC)


MASSIVE BLOOD TRANSFUSION IN LIVER RESECTION
Major complications of massive transfusion include:
- citrate toxicity
- acid-base abnormalities
- hypothermia
- hyperkalemia and hypocalcemia
- DIC (disseminated intravascular coagulation)

May be associated with a number of hemostatic and metabolic complications
Involves the selection of the appropriate amt and types of blood components to be administered.
- volume status
- tissue oxygenation
- management of coagulation abnormalities
- ionized calcium/potassium
- acid-base balance: metabolic alkalosis (citrate --> lactate --> HCO3)
- hemostasis
- hypotension d/t bradycardia (hypocalcemia decr contractility and rate)
contains 200 ml of RBC (2/3 cells; 1/3 Na citrate - 100 ml)
One unit of PRBC will raise Hct by 3-4% without continued bleeding
- O2 release at the tissue level by transfused RBCs is diminished compared with native red cells
- storage reduces 2,3 DPG (diphosphoglycerate) levels
- shift to the LEFT of the oxyhemoglobin dissociation curve during massive transfusion
- the transfused cells regenerate 2,3 DPG to normal levels within 6-24 hours after transfusion
HEPATIC RESECTION CASE STUDY
Key Points:
- most common cancers that arise in liver are d/t hepatocellular carcinoma and mets from colorectal cancer
- majority of hepatic rxns are performed for removal of cancerous tissue
- bleeding and hemorrhage are major risks associated with hepatic rxn
- epidural analgesia can be used to attenuate the stress response and decrease postop pain
1.5 kg
4 lobes: right, left, caudate, quadrate
*Classic description does not include internal features such as vessels and biliary duct branching that are vital for hepatic surgery
liver lobule: composed of hepatocytes, sinusoids, kupffer cells in trangular arrangement around central vein
Normal hepatic blood flow 1500 ml/min or 25-30% cardiac output
Functions performed by liver:
gluconeogenesis (glucose from AA, lactate, glycerol)
glucogenesis (glycogen from glucose)
glycogenolysis (glycogen to glucose)
cholesterol synthesis
lipogenesis (production of triglycerides)
clotting factors: I (fibrinogen), II (prothrombin), V, VII, IX, XI, protein C, S, antithrombin
storage for folate, glycogen, fat soluble vitamins (B12, ADEK), iron, copper
Hgb from RBC broken down to bilirubin and converted to biliverdin by liver to facilitate excretion
ammonia to urea
Hepatocellular Carcinoma (HCC):
AKA primary liver cancer or hepatomaprimarily caused by chronic HBV, HCV and cirrhosis d/t alcohol abuse
S&S:
initial - abdominal pain, unexplained weight loss
with cirrhosis - jaundice, ascites, esophageal varices, portal HTN
**In patients who have HCC WITHOUT cirrhosis - liver resection is treatment of choice.**
if patients have cirrhosis (as cause for HCC), liver rxn is limited --> high risk of postop liver failure
percutaneous ethanol injection and radiofrequency ablation may be an option for tx
Ultimately - liver resectability is judged by liver function, stage of liver CA and overall condition of pt.
Surgical Resection:
1. Segmental anatomic surgery: ligation of vasculature PRIOR to resecting liver parenchyma
2. Nonanatomic division of liver (wedge rxn): ligating and resecting vessels and ducts as they are encountered during rxn of parenchyma - only tumor with margin is removed
Preop Considerations:
- labs: elytes, glucose, LFTs, coags, CBC, T&C
- CXR, CT, ECHO, abdominal u/s
- Lines
- tx/optimize those who are coagulopathic by admin of blood products/antifibrinolytic meds
- prepare to admin RBCs and albumin
- rapid fluid infusing device in room
- epidural catheter
- 3D mapping
Methods to reduce blood loss:
- hemostatic stapling
- cavitron u/s surgical aspirator (CUSA) - ultrasonic dissection
- clamp crushing technique
- Pringle maneuver - occlusion of main blood vessels but can cause ischemia - 15-20 min clamp followed by 5 min reperfusion period
- total vascular occlusion - occlusion of arterial and venous flow to liver and out of liver
- managing CVP
Low CVP:
- achieved by fluid restriction, postural changes, vasodilators, diuresis
- CVP < 5 mmHg facilitates lower blood loss
- IV nitrolycerine and lasix
- Reverse T to decrease CVP
- Oliguria may occur but rate of postop renal failure does not incr when SBP is maintained > 90 mmHg
- at completion of liver rxn, volume resuscitation with crystalloid and albumin to normalize hemodynamic profile & discover areas of bleeding
- low CVP may incr risk for VAE * common occurrance with liver rxn - usually does NOT result in physiologic compromise
- 100% O2
- aspirate air via central line from RA
- T-berg and L lateral decub
- IV fluids
- vasopressors to incr BP
- ACLS prn
*can be done for CAs that are present on surface of liver where larger blood vessels are not affected
absence of larger incision, decr postop pain, decr LOS, decr recovery time
Intraop Period
- routine monitors, CVP
- Rx to reduce gastric volume and incr pH
- RSI with cricoid
- consider hemodynamic status prior to choosing induction agent
- NMBD that are non organ dependent metabolism
- N2O incr risk for VAE
- fentanyl and sufentanil are ok
- control BS
- hypothermia inhibits coagulation cascade & contributs to blood loss
- monitor coagulation: admin plts, FFP, cryo prn
- antifibrinolytics (aminocaproic acid and tranexamic acid) preop for procoagulation
- pain control: epidural or PCA +/-
- Postop complications: Hemorrhage, respiratory complications (atelectasis, effusion, PNA), e-lyte abnormalities, hypothermia, hypoglycemia, DIC
HOW I GOT CURED OF HERPES VIRUS.
ReplyDeleteHello everyone out there, I am here to give my testimony about a herbalist called Dr Imoloa. I was infected with herpes simplex virus 2 in 2013, I went to many hospitals for cure but there was no solution, so I was thinking on how I can get a solution out so that my body can be okay. One day I was in the pool side browsing and thinking of where I can get a solution. I go through many websites where I saw so many testimonies about dr imoloa on how he cured them. I did not believe but I decided to give him a try, I contacted him and he prepared the herpes for me which I received through DHL courier service. I took it for two weeks after then he instructed me to go for check up, after the test I was confirmed herpes negative. Am so free and happy. So, if you have problem or you are infected with any disease kindly contact him on email drimolaherbalmademedicine@gmail.com. Or / whatssapp --+2347081986098.
This testimony serve as an expression of my gratitude. He also has
herbal cure for, FEVER, BODY PAIN, DIARRHOEA, MOUTH ULCER, MOUTH CANCER FATIGUE, MUSCLE ACHES, LUPUS, SKIN CANCER, PENILE CANCER, BREAST CANCER, PANCREATIC CANCER, CHRONIC KIDNEY DISEASE, VAGINAL CANCER, CERVICAL CANCER, DISEASE, JOINT PAIN, POLIO DISEASE, PARKINSON'S DISEASE, ALZHEIMER'S DISEASE, BULIMIA DISEASE, INFLAMMATORY JOINT DISEASE CYSTIC FIBROSIS, SCHIZOPHRENIA, CORNEAL ULCER, EPILEPSY, FETAL ALCOHOL SPECTRUM, LICHEN PLANUS, COLD SORE, SHINGLES, CANCER, HEPATITIS A, B. DIABETES 1/2, HIV/AIDS, CHRONIC RESPIRATORY DISEASE, CARDIOVASCULAR DISEASE, NEOPLASMS, MENTAL AND BEHAVIOURAL DISORDER, CHLAMYDIA, ZIKA VIRUS, EMPHYSEMA, TUBERCULOSIS LOW SPERM COUNT, ENZYMA, DRY COUGH, ARTHRITIS, LEUKAEMIA, LYME DISEASE, ASTHMA, IMPOTENCE, BARENESS/INFERTILITY, WEAK ERECTION, PENIS ENLARGEMENT. AND SO ON.
website- www.drimolaherbalmademedicine.wordpress.com